
For some earlier stage cancers of the oesophagus (food pipe), surgery can be used to try to remove the cancer. If the cancer has not yet spread far beyond the oesophagus, removing part or all of the oesophagus (and nearby lymph nodes) may cure the cancer. Unfortunately, most oesophageal cancers are not found early enough for doctors to cure them with surgery. In those cases, surgery is often combined with other treatments, such as chemotherapy and/or radiation therapy.
What type of surgery do I need?
The type of surgery you need for cancer of the oesophagus depends on:
- The size of the tumour
- Where it is in your oesophagus.
Operations to remove some or most of the oesophagus (called oesophagectomies) are major surgery.
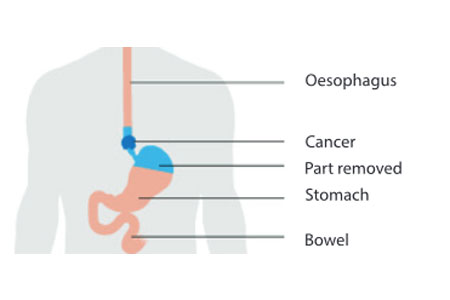
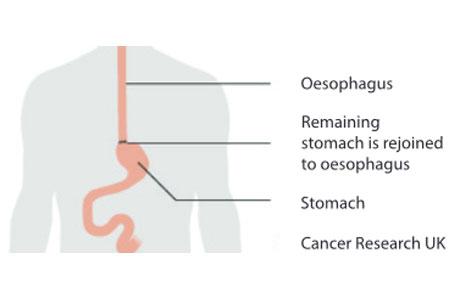
Removing part of the oesophagus and part of the stomach
If the cancer is in the lower part of the oesophagus (near the stomach) or at the place where the oesophagus and stomach meet, the surgeon will remove part of the stomach, the part of the oesophagus containing the cancer, and about 8 to 10 centimetres of normal oesophagus above this. This is an oesophagogastrectomy. Then the stomach is connected to what is left of the oesophagus either high in the chest or in the neck.
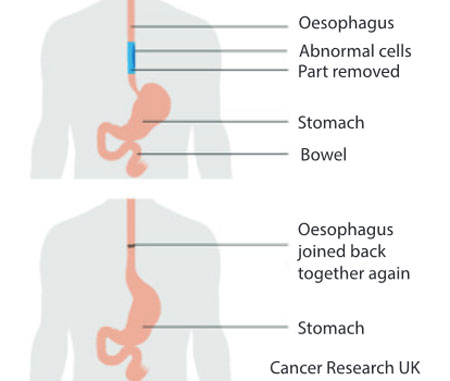
Removing part of your oesophagus and reattaching it to your stomach
This operation is for when the cancer is only in the oesophagus. The surgeon removes the cancer and some surrounding healthy tissue. They then rejoin the healthy part to your stomach and pull it up into the chest.
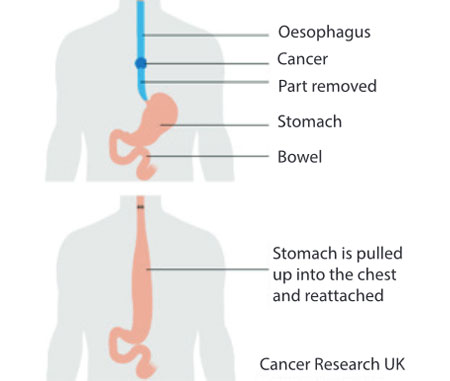
Removing all of your oesophagus
If the tumour is in the upper or middle part of the oesophagus, most of the oesophagus will need to be removed. This operation is a total oesophagectomy. Your surgeon uses your stomach or more rarely a piece of your bowel to replace the part of the oesophagus that they remove. When they use the stomach to replace the oesophagus the surgeon pulls your stomach up into your chest and connects it to the oesophagus in the neck.
How your surgeon does your operation
Oesophagectomy may be done using either of two main types of techniques. In the standard, open technique, the surgeon operates through one or more large incisions (cuts) in the neck, chest, or abdomen. In minimally invasive surgery, the surgeon operates through several smaller incisions using special long, thin surgical instruments.
Open oesophagectomy
Many different approaches can be used to remove part of the oesophagus:
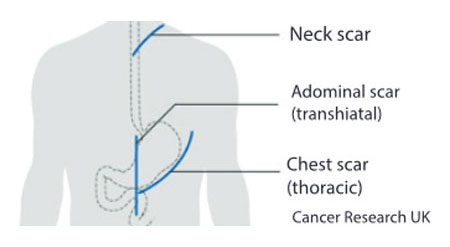
- For a transthoracic oesophagectomy, the oesophagus is removed with the main incisions in the abdomen and the chest;
- If the main incisions are in the abdomen and neck, it is called a trans-hiatal oesophagectomy;
- Some procedures are done through incisions in the neck, chest, and abdomen.
You and your surgeon should discuss in detail the operation planned for you and what you can expect.
Minimally invasive oesophagectomy
For some early (small) cancers, the oesophagus can be removed through several small incisions instead of large incisions. The surgeon puts a scope (like a tiny telescope) through one of the incisions to see everything during the operation. Then the surgical instruments go in through other small incisions. In order to do this type of procedure well, the surgeon needs to be highly skilled and have a great deal of experience removing the oesophagus this way. Because it uses smaller incisions, minimally invasive oesophagectomy may allow the patient to leave the hospital sooner and recover faster.
No matter which approach is used, oesophagectomy is not a simple operation, and it may require a long hospital stay.
Lymph node removal
During your operation the surgeon examines the oesophagus and surrounding area. They take out all of the lymph nodes from around your oesophagus. This is a lymphadenectomy.
The surgeon takes out lymph nodes in case they contain cancer cells that have spread from the main cancer. Taking the nodes out reduces the risk of your cancer coming back in the future. It also helps your doctor to decide if you need chemotherapy after your surgery.
The number of lymph nodes your surgeon removes varies. Your surgeon might remove nodes from around your stomach as well.
Risks and side-effects of oesophagectomy
Like most serious operations, surgery of the oesophagus has some risks. Some complications from this surgery can be life-threatening.
- Short-term risks include reactions to anaesthesia; excess bleeding, blood clots in the lungs or elsewhere, and infections. Most people will have at least some pain after the operation, which can usually be helped with pain medicines.
- Lung complications are common. Pneumonia may develop, leading to a longer hospital stay, and sometimes even death.
- Some people might have voice changes after the surgery.
- There may be a leak at the place where the stomach (or intestine) is connected to the oesophagus, which might require another operation to fix. This is not as common as it used to be because of improvements in surgical techniques.
- Strictures (narrowing) can form where the oesophagus is surgically connected to the stomach, which can cause problems swallowing for some patients. To relieve this symptom, these strictures can be expanded during an upper endoscopy procedure.
- After the operation, the stomach may empty too slowly because the nerves that control its contractions can be affected by surgery. This can sometimes lead to frequent nausea and vomiting.
- After surgery, bile and stomach contents can enter the oesophagus because the muscle that normally controls this (the lower oesophageal sphincter) is often removed or changed by the surgery. This can cause symptoms such as heartburn. Sometimes antacids or motility drugs can help relieve these symptoms.
Surgery for palliative care
Sometimes minor types of surgery are used to help prevent or relieve problems caused by the cancer, instead of trying to cure it. For example, minor surgery can be used to place a feeding tube directly into the stomach or small intestine in people who need help getting enough nutrition.


