
Table of contents
- What is transarterial chemoembolisation?
- Why do I need TACE?
- Who can have a TACE procedure?
- What are the benefits of TACE?
- Who has made the decision?
- How do I prepare for TACE?
- Who will perform the procedure?
- What happens during TACE?
- Will it hurt?
- How long will it take?
- What happens afterwards?
- Are there any risks?
- What happens after the treatment has been completed?
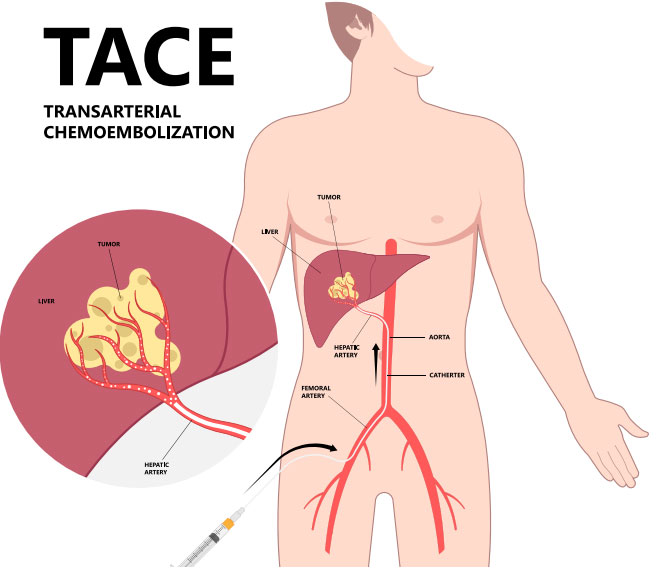
What is transarterial chemoembolisation?
Transarterial chemoembolisation or TACE is a palliative treatment for liver cancer. This can be a cancer originating in the liver or a cancer that has spread (metastasised) to the liver from other areas of the body.
TACE is a non-surgical and minimally invasive procedure performed by an interventional radiologist. Anti-cancer drugs (chemotherapy) are injected directly into the blood vessel feeding the cancerous tumour. In addition, synthetic material called embolic agents (small plastic beads) are placed inside the same blood vessels to cut off the tumour’s blood supply and trap the chemotherapy within. Therefore, TACE works in 2 ways:
- It gives high doses of chemotherapy to the tumour (to destroy cancer cells);
- It reduces the blood supply to the tumour and so starves it of oxygen and the nutrients it needs to grow.
Why do I need TACE?
Patients who have been referred for this procedure have tumours in the liver.
TACE is used most often to treat a cancer arising in the liver (primary liver cancer), called hepatocellular carcinoma (HCC) which is a cancer that occurs most often in people with chronic liver diseases, such as cirrhosis caused by hepatitis B or hepatitis C infection.
TACE can also be used to treat cancer that started in another area of the body but has spread to the liver, secondary liver cancers that can be treated by TACE include:
- Cholangiocarcinoma (primary cancer of the bile ducts in the liver)
- Colon cancer
- Breast cancer
- Neuroendocrine tumours
- Islet cell tumours of the pancreas
- Ocular melanoma
TACE is a palliative treatment, usually used to control the cancer, rather than cure it. The goal of TACE is to shrink the tumour and stop it growing. TACE may be used as a stand-alone treatment or in combination with surgery, chemotherapy, radiotherapy or radiofrequency ablation.
Depending on the type of cancer, its size and location, you may need to have several TACE sessions in order to control the cancer. For example, if there is a tumour on both lobes of the liver, one side will be treated first and after one month you will return to the hospital for an additional TACE procedure.
Around 70% of patients will see improvement after TACE, which has few side effects and can be used in combination with other treatments.
Who can have a TACE procedure?
Unfortunately, not everyone with a liver cancer can have this procedure. Your liver must be working well enough in order to withstand both the chemotherapy and the ‘blocking-off’ of the blood supply to the cancer within the liver. Other contraindications include portal vein thrombosis, previous severe contrast allergy, renal impairment or coagulopathy.

What are the benefits of TACE?
The purpose of TACE is to provide relief of symptoms related to the tumour, to reduce the size or rate of growth of the tumour and to improve your life expectancy. Studies from around the world have shown that TACE can be successful in controlling the cancer that is in your liver and delays the cancer progressing, so these patients with primary liver cancer who undergo the procedure live longer.
You may also be offered TACE to keep a liver tumour small if you are waiting for a liver transplant (it’s called ‘bridging’ therapy).
Who has made the decision?
The decision was taken during a ‘Tumour Board’ meeting during which specialists, including gastro-enterologists, general surgeons, oncologists, interventional radiologists, have discussed your case and have agreed on the treatment plan. However, you will also have the opportunity for your opinion to be considered and if, after discussion with your doctors, you no longer want the procedure, you can decide against it.
How do I prepare for TACE?
Before the procedure, your doctor will require blood tests to make sure that your liver and kidneys are working and to check that your blood is clotting normally. You will need a contrast-enhanced CT or an MRI scan performed in the 30-60 days before the procedure. You should inform your doctor of all the medications that you are taking. If you have any allergies or have previously had a reaction to the dye (contrast agent), you must tell the radiology staff before you have the test. Your doctor may advise you to stop some medications before the procedure. You must inform your doctor if there’s a chance you might be pregnant.
You may be asked not to eat for 4 hours before the procedure, although you may still drink clear fluids such as water.
Who will perform the procedure?
Specially trained doctors called interventional radiologists. Interventional radiologists are trained to perform various minimally-invasive procedures using medical imaging guidance, to diagnose, treat, and cure many kinds of conditions. They make small incisions and use needles and catheters to treat conditions inside your body.
The procedure takes place in a specialised X-ray room called a Cath-lab.

What happens during TACE?
You will be hospitalised in the day ward of the hospital. You will be asked to get undressed and put on a hospital gown. You will be taken into the Cath-lab room and connected to monitors that will track your heart rate, blood pressure and pulse during the procedure. You will be given sedation and medications will be given to prevent and treat nausea and/or pain.
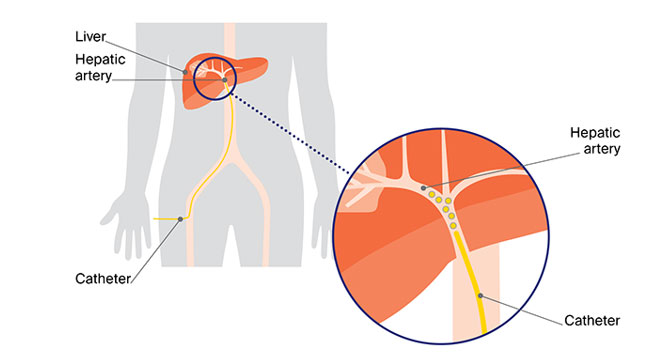
After giving local anaesthesia to the skin, the interventional radiologist will first pass a needle, then a wire into an artery in your groin. A small catheter (hollow tube) will then be moved forward over the guidewire into your artery under X-ray guidance in order to reach the liver and the arteries supplying the tumour.
A liquid (contrast) will be injected through the catheter to make the arteries visible on screen, so that the interventional radiologist can guide the catheter to the arteries supplying the tumour. You will be asked to hold your breath for a few seconds every so often throughout the procedure to ensure the pictures taken are clear. Once a small catheter is advanced in the artery supplying the tumour, the chemotherapeutic/embolic agent mixture will be injected.
At the end of the procedure the catheter is removed and site of access will be sealed. You will be asked to stay in bed for a few hours in order to reduce the potential for bleeding from the artery that was punctured.
Will it hurt?
When the local anaesthetic is injected, it will sting for a short while, but this soon wears off. You may feel a warm sensation for a few seconds when the contrast is injected.
How long will it take?
Every patient is different, and it is not always easy to predict; however, expect to be in the Cath-lab for about 1 to 2 hours.
What happens afterwards?
You will be taken back to day ward. Nursing staff will carry out routine observations including pulse and blood pressure and will also check the treatment site. You will generally stay in bed for a few hours, until you have recovered. Assuming you are feeling well, you will normally be discharged at the same day.
Are there any risks?
TACE is a safe procedure, but as with any medical procedure there are some risks and complications that can arise. The overall risk of a problem requiring further treatment is low (1–2%).
- You may have some bruising at the puncture site. This may be sore for a few days but will resolve.
- Most patients experience what is called post-embolisation syndrome. Symptoms include pain, nausea and slight fever or chills which can make you feel like you have a cold or a flu. Pain occurs because the blood supply to the tumour is blocked. These symptoms are usually easily managed with medications, and may take 1–2 weeks to settle.
- Very rare complications include: bleeding or blockage of the artery requiring treatment with a further procedure, infection in the liver requiring antibiotics, acute liver failure and non-target embolisation (injection of the drug/embolic into the arteries outside of the tumour).
You should call your doctor if:
- Your leg becomes pale and cold
- You notice redness, swelling, bleeding, or drainage at the puncture site
- You have pain that suddenly gets worse or changes in any other way
- You experience frequent diarrhoea
- You have significant shortness of breath
- You have a fever of 38°C or higher.
What happens after the treatment has been completed?
A CT scan or MRI of your liver will be performed about 4–6 weeks after the procedure to assess the response to treatment and also to assess the need for any further treatment. CT scans or MRI will be performed every 3 months thereafter to determine how much the tumour(s) ultimately shrink, and to see if and when any new tumour arises in the liver.
TACE can be repeated many times over the course of many years, as long as it remains technically possible and you continue to be healthy enough to tolerate repeat procedures.


