
Table of contents
What is a hysterectomy?
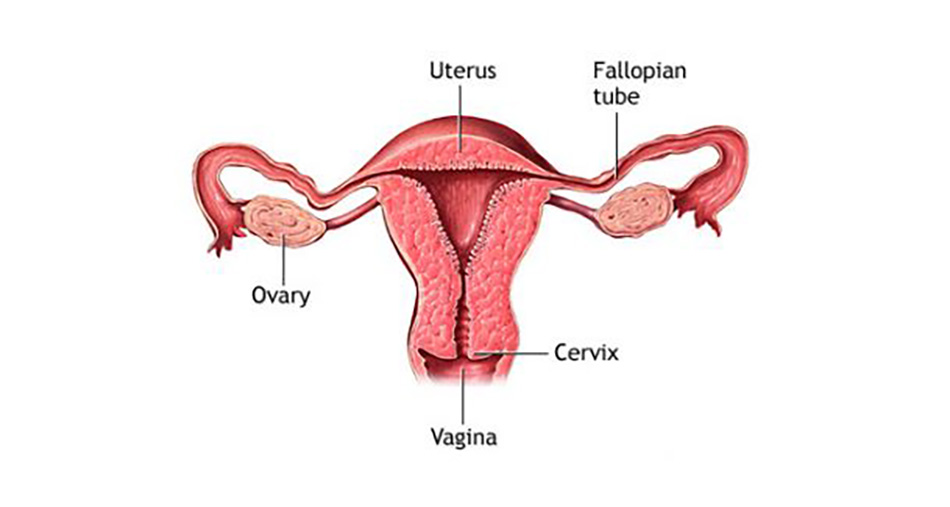
A hysterectomy is an operation to remove your womb (uterus).
Why is hysterectomy done?
Hysterectomy is used to treat several women’s health conditions including:
- Uterine fibroids
- Gynaecologic cancer
- Adenomyosis
- Endometriosis
- Uterine prolapse
- Chronic pelvic pain
- Abnormal uterine bleeding.
For most of these conditions, with the possible exception of cancer, hysterectomy is just one of several treatment options. You might not need to consider hysterectomy if medications or less invasive gynaecological procedures manage your symptoms.
You cannot become pregnant after a hysterectomy. If you are not sure that you are ready to give up your fertility, explore other treatments.
What is removed during hysterectomy?
There are different types of hysterectomy. Which hysterectomy is best for you will depend on the reason for the surgery, your age, your overall health, and other factors:
- Total hysterectomy, where both the uterus and cervix (neck of the womb) are removed. Fallopian tubes are usually also removed (bilateral salpingectomy);
- Subtotal hysterectomy, where just the uterus is removed and the cervix is not;
- Hysterectomy with salpingo-oophorectomy (removal of one or both or your ovaries and your fallopian tubes) at the same time.
Salpingo-oophorectomy results in what is known as surgical menopause. With surgical menopause, menopause symptoms often begin suddenly for women after having the procedure done. Depending on how much these symptoms affect your quality of life, you may need short-term treatment with hormones.
What are the different ways hysterectomy can be performed?
There are three ways to remove the uterus:
- Vaginal hysterectomy: the removal of uterus and closing of the wound is performed through the vagina. There is no cut in the abdomen;
- Abdominal hysterectomy: the uterus is removed through a cut in the lower abdomen. The cut is about 15–20 cm in length and runs across your abdomen, usually below the bikini line. Less commonly, it may be necessary to have a vertical cut that runs from the belly button down to the pubic area;
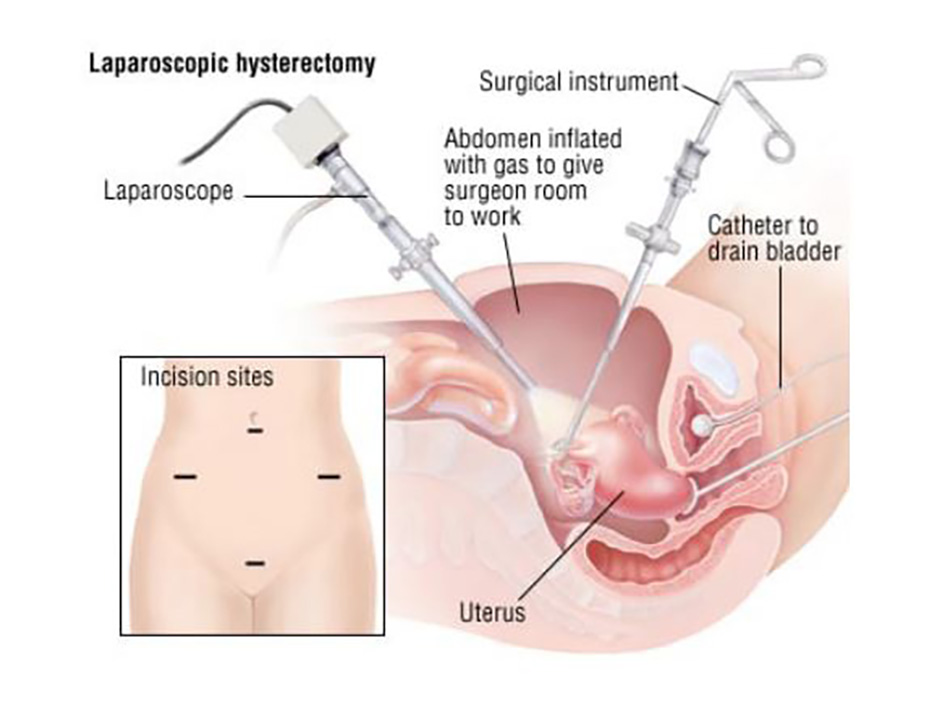
- Laparoscopic hysterectomy: about four small keyhole cuts are made in the abdomen to divide the attachments of uterus, ovaries and tubes in the pelvis. The uterus is usually then removed through the vagina.
Laparoscopic hysterectomy is preferred by many surgeons because it results in shorter duration of hospitalisation, less pain, fewer complications, and more rapid return to normal activities than abdominal hysterectomy. Vaginal hysterectomy is less often performed but is a good option in selected patients. Ultimately, the choice between the three techniques depends on the reason for the surgery, if there is a history of previous abdominal surgical procedure, the patient’s age, and other parameters.
What are the risks of a hysterectomy?
A hysterectomy is generally very safe, but with any major surgery comes the risk of complications. They include:
- Damage to the bladder or ureter (tube from kidney into bladder)
- Haemorrhage requiring blood transfusion
- Damage to the bowel
- Return to theatre due to bleeding or due to wound problems
- Pelvic abscess or infection
- A blood clot in leg or lung can occur
- Earlier onset of menopause even if the ovaries are not removed.
Some complications may mean that further treatment or surgery is required.
What to expect?
Before the procedure
You will see an anaesthesiologist at least 48 hours before your procedure. You will have the opportunity to ask any questions about the anaesthesia and about pain relief after your operation. He/she will give you printed instructions on how to prepare for your surgery.
You will be hospitalised the day before your surgery. The day before and morning of your surgery, you will be instructed to shower with an antibacterial soap to reduce the risk of infection.
You will usually be given a general anaesthetic to put you to sleep during the operation. The procedure itself generally lasts about one to two hours, although you’ll spend some time beforehand getting ready to go into the operating room.
After the procedure
After the surgery, you will spend a couple of hours in the recovery room to make sure everything is fine before going into your room.
Most women experience some pain for the first few days and you will be given painkillers to help with this. You also will be given medications to prevent blood clots. The urinary catheter will be removed about 12 or 24 hours after the surgery and you will be able to eat a few hours after being in your room. You may have some vaginal bleeding and will need to wear a sanitary pad.
Most women will stay in the hospital 2-4 nights after the hysterectomy but it could be longer. Your exact day of discharge will depend on the reasons for your operation, your general health and how smoothly things go after surgery.
When you go back home
Be sure to get plenty of rest, even if you need to move around as much as you can.
Until six weeks after surgery:
- Do not lift anything heavy;
- Avoid inserting anything into the vagina to allow time for healing to take place (e.g. use sanitary pads and not tampons);
- Do not have vaginal intercourse.
Come back to hospital if:
- Your wound becomes red or inflamed, painful;
- You have fever higher than 38°C;
- You have heavy vaginal bleeding, heavier than a normal period;
- You have offensive vaginal discharge;
- You have pain that is not relieved by simple analgesia, particularly abdominal pain;
- You are having difficulty passing urine or a burning, stinging feeling when you pass urine;
- You experience leg pain or swelling.
Life after a hysterectomy
A hysterectomy permanently changes some aspects of your life. For instance:
- You’ll no longer have menstrual periods;
- Most of the time, you’ll get relief from the symptoms that made your surgery necessary;
- You won’t be able to become pregnant;
- If you’re premenopausal, having your ovaries removed along with a hysterectomy starts menopause;
- If you have a hysterectomy before menopause and you keep your ovaries, you may experience menopause at a younger than average age;
- If you have a partial hysterectomy, your cervix remains in place, so you’re still at risk of cervical cancer. You need regular Pap tests to screen for cervical cancer.
Other parts of your life will likely return to normal or perhaps improve once you’ve recovered from your hysterectomy. For example:
- If you had a good sex life before a hysterectomy, chances are you’ll maintain it afterward. Some women even experience more sexual pleasure after a hysterectomy. This may be due to relief from the chronic pain or heavy bleeding that was caused by a uterine problem;
- The relief of symptoms may greatly enhance your quality of life. You may have an improved sense of well-being and a chance to get on with your life.
On the other hand, you may feel a sense of loss after hysterectomy. Premenopausal women who must have a hysterectomy to treat gynaecologic cancer may experience grief and possibly depression over the loss of fertility. If sadness or negative feelings begin to interfere with your enjoyment of everyday life, talk with your doctor.


