
WHAT IS A KIDNEY STONE?
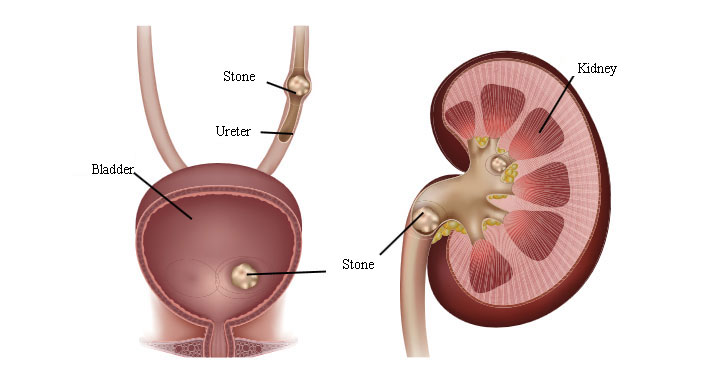
A kidney stone is a hard, solid mass that can form after minerals or acid salts in your urine have crystallised. Kidney stones develop in the kidney and either stay there or move to the ureter. Most stones are small and are flushed out in the urine. Some grow over many years to become quite large. Sometimes stones get stuck in the ureter, block the normal flow of urine, and cause symptoms. Stones can also be too big to leave the kidney. In both cases, you may need treatment to remove them. There can be one or more stones present at any one time. Anyone can get a kidney stone. They affect up 12% of men and 5% of women during their lifetime. Most occur between the ages of 20 and 60. Some people keep getting kidney stones throughout their lives.
WHAT CAUSES A KIDNEY STONE?
The most common cause of urinary stones is the imbalance in the composition of urine. This may be connected to how much you drink and whether there are substances in your urine which trigger stone formation or deficiency of some substances which prevents stone formation. Some conditions can cause kidney stones:
- Certain urological conditions like ureteropelvic junction obstruction, polycystic kidney disease, nephrocalcinosis, vesico-ureteric reflux, ureteral stricture, tubular ectasia, etc.
- Renal tubular acidosis
- Hyperparathyroidism
- Some gastro-intestinal conditions like Crohn’s disease, chronic diarrhoea, malabsortion and bariatric surgery
- Sarcoidosis
- Also, urinary tract infections can lead to stone forming.
The urinary tract However, for most people with stones, the exact cause is not found. Kidney stones form when your urine contains more crystal-forming substances — such as calcium, oxalate and uric acid — than the fluid in your urine can dilute. At the same time, your urine may lack substances that prevent crystals from sticking together, creating an ideal environment for kidney stones to form. Stones can be made up of different matters. The most common ones are made up of calcium. There are also uric acid stones, ammonium urate stones, struvite stones (that form in response to a urinary tract infection), and cystine stones (that form in people with a hereditary disorder called cystinuria). Specific blood and urine tests called “metabolic evaluation” may be necessary to understand the composition of urine for preventive measures such as adjusting your diet.
WHAT ARE THE SYMPTOMS OF KIDNEY STONES?
People often associate kidney and ureteral stones with pain. However, symptoms can vary from severe pain to no pain at all, depending on stone characteristics – such as the size, shape, and location of the stone in the urinary tract.
- No symptoms: some stones do not cause any discomfort or clinical problems. These are called asymptomatic stones and are usually small. In general, asymptomatic stones are found during X-ray, ultrasound or in any other imaging procedures for other conditions.
- Non-visible blood in your urine, found only when your urine is tested using a sensitive dipstick.
- A urinary tract infection may occur when bacteria become trapped in urine that pools above a blockage.
- Stones that do not block the ureter completely can cause a recurrent, dull pain in the flank.
- Acute renal colic.
ACUTE RENAL COLIC
- It is due to a stone passing down towards your bladder from your kidney. If it becomes lodged in the ureters, it may block the flow of urine and cause the kidney to swell and the ureter to spasm, which can be extremely painful.
- It usually starts by a severe, sharp pain in your loin, below the ribs, that comes in waves, fluctuates in intensity and does not decrease if you change position. The pain may radiate to the lower abdomen and groin or testicles/labia as the stone moves down.
- Often coupled with nausea and vomiting.
- When the stone gets close to your bladder, you may get a constant need to pass urine although there is nothing to pass; this is due to the stone irritating the base of your bladder.
- A stone in this position can also cause:
- Burning when you pass urine;
- Pain at the tip of your penis or urethra;
- Visible blood in your urine.
- Fever and chills means that an infection is present which requires decompression (see below) and antibiotics.
An attack may last many hours. This often settles when the stone has passed into your bladder, which may take some time.
TREATMENT OF ACUTE RENAL COLIC
Acute renal colic is a medical emergency. Pain is usually relieved with non-steroidal anti-inflammatory drugs. If this first step of treatment does not help, you will get stronger pain killers called opioids. Usually, they are injected directly into the vein. Intravenous lidocaine is quite effective for intractable renal colic unresponsive to standard therapy and typically starts to work in 3-5 minutes. The protocol is to inject lidocaine 120 mg in 100 mL normal saline intravenously over 10 minutes for pain management. On a rare occasion, drugs do not work. In this case, the doctor may need to drain urine from your kidney. This is called decompression.
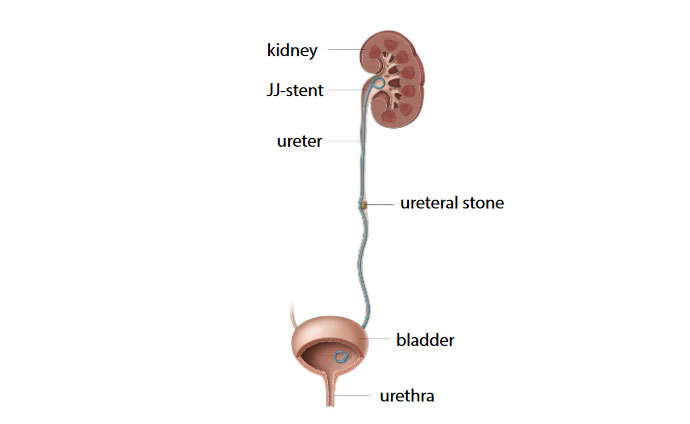
A JJ-stent is inserted to make sure urine can flow through the urinary tracThere are two methods of decompression:
- By placing a ureteral JJ-stent in your ureter through your urethra;
- By inserting a tube into your kidney directly through the skin (a percutaneous nephrostomy).
Both methods are equally effective.
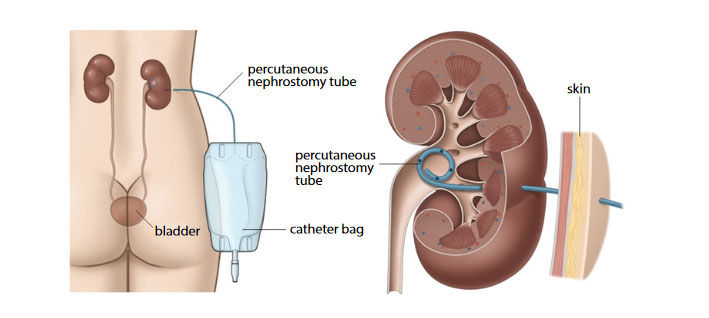
Percutaneous nephrostomyInvestigations will include:
- A urine test to look for infection, blood and crystals;
- Blood test to check your blood cell count and how your kidney is working;
- Imaging: pain relief must not be delayed by imaging assessments, but when the pain is sufficiently controlled a CT scanner of the abdomen and pelvis will be performed to diagnose the stone, determine its location and size and its impact on the urinary tract. Ultrasound, a noninvasive test that is quick and easy to perform, is another imaging option to diagnose kidney stones.
If the acute renal colic is associated with fever you will get blood and urine tests to check if you have an infection, in that case urgent decompression, usually by a double-J stent, is indicated.
WHAT TO EXPECT AFTER A RENAL COLIC
Most people will pass the kidney stone without any trouble in the next few days to weeks. The time it takes to pass a stone varies from person to person. You can help this process by drinking plenty of water to increase the flow of urine and taking your prescribed pain killers regularly. Your doctor may also prescribe what is called “medical expulsive therapy”. This type of medication, known as an alpha blocker (for example dutasteride, tamsulosin and alfuzosine), relaxes the muscles in your ureter, helping you pass the kidney stone more quickly and with less pain. Each time you urinate, do so in a jar. Pour the urine from the jar through the strainer and into the toilet. Continue doing this until 24 hours after your pain stops. By then, if there was a kidney stone, it should pass from your bladder. Some stones dissolve into sand-like particles and pass right through the strainer. In that case, you may never see a stone. Save any stone that you find in the strainer and bring it to your doctor for analysis. It may be possible to prevent certain types of stones from re-forming. Therefore, it is important to know what kind of stone you have. Try to stay as active as possible since this will help the stone pass. Do not stay in bed unless your pain prevents you from getting up. You may notice a red, pink or brown colour to your urine. This is normal while passing a kidney stone.
WHEN TO SEEK URGENT MEDICAL ATTENTION AFTER A RENAL COLIC
You should come back to the hospital without delay if:
- You have a high temperature of 38° or over;
- You have an episode of shivering or shaking;
- The pain gets worse, particularly if it’s a sudden, severe pain;
- You are unable to pass urine.
LONG-TERM TREATMENT AND PREVENTION
After the acute renal colic you will be referred to a specialist of urinary tract diseases and conditions, called an urologist, who will decide if further investigations and treatment are necessary, which may include:
- Extracorporeal Shock Wave Lithotripsy (described in another FV Hospital brochure), percutaneous nephrostomy or ureteroscopy: they may be required for kidney stones that are too large to pass on their own;
- Analysis of the type of stone;
- Investigations to determine a possible cause;
- Specific prevention measures adjusted to the type of stone including changes in your diet.
If you have had a kidney stone, there is strong possibility you will have another kidney stone in the future. Drinking more is recommended with any stone type:
- Make sure you drink 2.5 to 3 litres every day;
- Drink evenly throughout the day;
- Drink even more if you live in a hot climate or do a lot of physical exercises.
Related Articles
Related Articles
Adult Circumcision
What is circumcision? Circumcision is the surgical removal of the foreskin. The foreskin covers the head of a flaccid penis. When the penis is erect, the foreskin pulls back to reveal the penis. Why is it done? Many adult men and teens seek circumcision for medical, health, sexual, cultural, religious and cosmetic reasons. Circumcision is […]
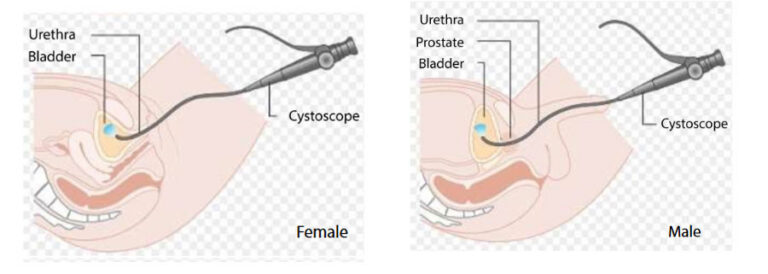
Cystoscopy
WHAT IS CYSTOSCOPY? This procedure is used to examine your bladder. Your doctor will insert a cystoscope, which is a thin tube with a camera and light on the end, through your urethra (which is the tube that collects urine from your bladder to the outside of your body) and into the bladder. Small surgical […]

Percutaneous nephrolithotomy
Some people are prone to stones forming in the kidney. Some of these do not give you any problems while others, if left untreated may grow and cause damage to the kidneys. Urine is made by the kidneys and drains via narrow tubes called ureters into your bladder where it is stored until you empty […]

Percutaneaous kidney biopsy under image guidance
What is percutaneous kidney biopsy? A kidney biopsy, also called renal biopsy, is a procedure to remove a small piece of kidney tissue so that it can be examined under a microscope for signs of damage or disease. Your doctor may recommend a kidney biopsy if blood tests, urine tests or imaging techniques don’t provide […]
Adult Circumcision
Cystoscopy
Percutaneous nephrolithotomy
