
Table of contents
This document has been conceived under the authority of the French Society of Plastic Reconstructive and Aesthetic surgery (Société Française de Chirurgie Plastique Reconstructrice et Esthétique – SOFCPRE) to complete the information that you received in your first consultation with your Plastic Surgeon. It aims to answer all the questions that you might ask, if you decide to undertake thigh inner side lifting. The aim of this document is to give you all the essential information you need in order to make an informed decision, with full knowledge of the facts related to this procedure. Consequently, we strongly advise you to read it carefully.
DEFINITION, OBJECTIVES AND PRINCIPLES
Where there is a loosening of the skin at the inner thighs, liposuction alone is not enough and only a tightening of the skin may correct this defect: this is the medial thigh lifting or lifting of the inner side of the thigh.
This intervention is then designed to remove the excess of skin, reduce the underlying fatty infiltration and suspend the skin from the deeper tissues (to the underlying aponeurotic plane).
These lesions do not justify an assumption by health insurance, excluding when they are effects of obesity (after bariatric surgery) that may, under certain conditions, be covered by health insurance.
BEFORE SURGERY
A preoperative assessment is normally conducted as required.
The anaesthesiologist will be seen in consultation at the latest 48 hours before surgery.
Smoking cessation is strongly recommended at least one month before and one month after the intervention (smoking can cause a delay of healing).
No medication containing aspirin should be taken within 10 days prior to surgery.
A skin preparation is usually prescribed the day before and the morning of surgery.
TYPE OF ANAESTHESIA AND HOSPITAL STAY
Type of anaesthesia: The lifting of the inner thighs can be done under general anaesthesia or under local anaesthesia deepened by intravenous tranquilizers (“vigil” anaesthesia).
The choice between these different techniques will be the result of a discussion between you, the surgeon and the anaesthesiologist.
Hospital stay: The average hospitaL stay is 1 to 3 days depending on the case.
THE PROCEDURE
Each surgeon adopts his/her own technique that he/she adapts to each case in order to obtain the best results. However, some common basic principles apply:
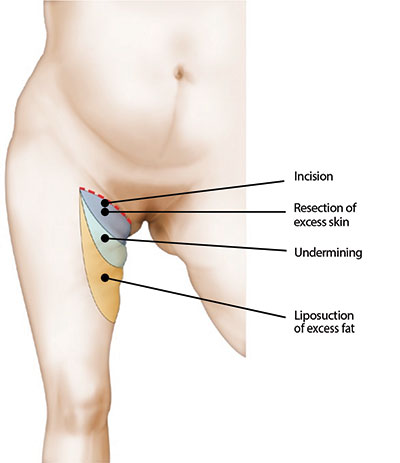
The incision is located in front near the groin. It then extends into the groove between the perineum and the upper inner thigh, and goes back to the gluteal fold where it ends. This incision corresponds to the future scar.
In some cases a vertical scar, more or less long, is associated at the inner side of thighs.
Liposuction is associated whenever there is a fatty infiltration of the region.
Excess skin is removed as necessary, and a fixation is performed in depth in the ligament located at the top of the inner side of the thigh, in order to properly maintain the correction of the collapse, so that the scar does not go back down and ensure the continuity of a normal and harmonious anatomy. The scar is well hidden in a natural crease and will be fairly inconspicuous.
At the end of the surgery, either a dressing made with sticky elastic bands or liposuction stockings will be placed.
The duration of the intervention is, on average, an hour and a half, but it varies depending on the surgeon and the extent of improvements to be made.
AFTER OPERATION: POST-OPERATIVE EFFECTS
- The discharge will usually be the next day or two days after the surgery.
- In the postoperative, bruising (bruises) and edema (swelling) can occur. They regress in 10-20 days after surgery.
- The pain is usually minor, limited to a few phenomena of tightness and shooting pain.
- The healing period can be a bit uncomfortable because of the tension on the edges of the suture.
- Any sudden movement of stretching should be avoided.
- There should be a work leave of 1 to 3 weeks, depending on the nature of the work.
- The practice of a sport can be resumed gradually from the sixth postoperative week.
- The scar is often pink during the first 3 months, and then it usually fades after the 3rd month, and this gradually over 1-3 years.
- The scar should not be exposed to sunlight or UV before three months after surgery.
THE RESULT
It is appreciated within 6 to 12 months after surgery.
There is, most often, a good correction of the fatty infiltration and sagging skin, which significantly improves the morphology of the thigh.
The scars are usually discrete, especially since they are hidden in a natural crease.
Thus, thanks to improved techniques and experience, the results of this intervention, which has had a bad reputation for a long time , have improved greatly today.
The goal of this surgery is to bring improvement and not to achieve perfection. If your wishes are realistic, the result should give you great satisfaction.
It is nevertheless a delicate surgery that is not in any way immune to a number of imperfections or even complications.
DISAPPOINTING RESULTS
In most cases, a lifting of the inner thighs correctly indicated and performed makes a real service to the patients obtaining a satisfactory result and consistent with what was expected.
However, it is not uncommon for localized imperfections to be observed, even they are not real complications:
- These imperfections notably include the scar, that can be a little too visible, stretched, or adherent. If excessive tension was placed on the sutures, we can observe a traction or even a downward migration of the scar, exposing the risk of traction on the vulva. We also know that if the scars fade well in general with time, they do not disappear completely. In this regard, we must not forget that, if the surgeon performs the sutures, the scar itself is the fact of the patient.
- These scars are subject to the hazards of any healing with the risk of hypertrophic changes, which require specific treatment.
- The results of liposuction can be characterized by a lack of correction, a slight residual asymmetry or small surface irregularities.
These imperfections are generally accessible to further treatment, small surgical “re-touches” performed under local anaesthesia or local anaesthesia with sedation, but not before the sixth month after surgery.

POSSIBLE COMPLICATIONS
An inner thigh lift, although carried out essentially for aesthetic reasons, none the less is a real surgery, which involves the risks associated with any medical procedure, however small it may be.
We must distinguish complications from anaesthesia and those associated with surgery:
- Regarding anaesthesia, during the consultation, the anaesthesiologist will inform the patient about his/ her anaesthetic risks. You should know that anaesthesia induced reactions in the body are sometimes unpredictable and more or less easy to control: the fact of using a fully qualified anaesthesiologist practicing in a real surgical context make surgical risk become statistically almost negligible.
- Be aware, in fact, that the anaesthesia drugs and techniques, and monitoring methods have made tremendous progress over the last twenty years, providing optimal safety, especially when the procedure is performed not as an emergency and in a healthy person.
- Regarding the surgical procedure, choosing a qualified and competent Plastic Surgeon, trained for this type of intervention, limit the risks at maximum, although not abolish them completely.
In fact, complications are possible after an inner thigh lift, which is one of the most delicate operations of plastic and aesthetic surgery.
Among these possible complications, we should mention:
- Thrombo-embolic accidents (blood clots, pulmonary embolism), although generally rare after this type of intervention, are among the most fearsome. Preventive measures should minimize their severity impact: wearing of anti-thrombosis stockings, early get-up and walking, and possibly anti-coagulant treatment.
- The occurrence of a hematoma, in fact quite rare, can justify its evacuation in order to avoid the risk of altering the aesthetic quality of the outcome.
- The occurrence of infection is favoured by the proximity of natural orifices; its treatment involves surgical drainage and prescription of antibiotics.
- Sometimes can be observed from the 8th postoperative day, the occurrence of an effusion associated with a lymph flow: such effusion may need to be punctured and usually resolves without particular consequences.
- Delayed healing can sometimes be observed, leading to longer postoperative course.
- Skin necrosis is rarely seen: it is usually limited and localized. The prevention of that necrosis depends on a correct indication and the performance of an adapted and prudent surgical technique.
- Alterations in sensibility, including reduced sensibility of the upper part of the inner side of the thigh can be observed: usually the normal sensitivity returns with a delay of 3 to 6 months after the operation.
All things considered, the risks must not be overestimated, but you must be conscious that an operation, even a minor one, always has some degree of unforeseeable unknown factors.
You can be assured that if you are operated on by a qualified Plastic Surgeon, he will have the experience and skill required to avoid these complications, or to treat them successfully if necessary.


